갑상선 석회화 결절은 암일 가능성이 높습니까?
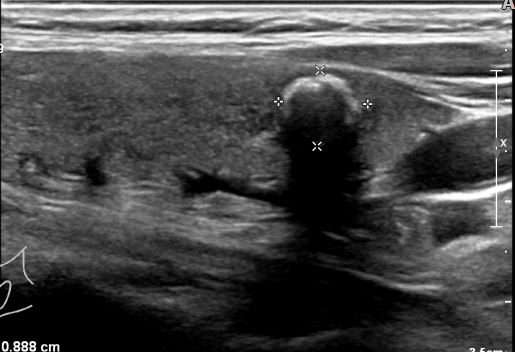
갑상선 거대석회결절(macr ocalcification)
학생 때 그렇게 배웠어요갑상선에 가장 일반적인 유형인 유두상암에 흔히 나타나는 소견이 석회화(미세석회화;microcalcification)라고 하는 것으로 갑상선에 석회화 결절은 암일 가능성이 높기 때문에 반드시 세포검사를 하도록
그럼 갑상선에 석회화 결절이 있다고 하면, 암의 확률은 어느 정도일까요?
인기글



")
One of the most important ultrasound features of cancer is the presence of calcifications , especially microcalcifications , in a thyroid nodule . The presence of microcalcifications on an ultrasound is felt to be highly suggestive of thyroid cancer . Since calcifications can also be seen in benign thyr … www.thyroid.org
재미있는 논문이 있어서 가져와봤어요.
- 초음파상 석회가 보여도 조직검사상 석회가 나온 경우는 절반밖에 없는 2.12.8%는 초음파상 석회가 없는데 조직검사상 석회가 있었다.3. 석회가 있는 경우 (미세석회화인지 큰 석회결정인지 관계없이) 54%에서 암이 발견됐다.4.45%는 초음파상 석회가 없었음에도 암이 발견됐다.5. 초음파상 석회가 있는지 없는지는 암 발견율에 관계가 없었다.6. 초음파상 미세석회화가 있는 54%에서 암이 발견되었는데, 이는 거대석회결절과 그 비율에 차이가 없었다.
이 논문이 암시하기를, 석회화는 신뢰할 수 있는 ‘암의 결정적 징후’가 아니라는 것, 특히 미세석회화(microcalcification)가 암과 강한 관련이 있다는 상식은 상식이 아니라는 것입니다.
따라서 저자는 갑상선암을 진단할 때 다양한 상황을 고려해야 한다고 주장하고 있습니다.임상적 양상, 과거사, 영상학적 이미지, 가족력 등 단순히 석회화 하나만으로 단정짓지 말아달라는 것입니다.
하지만 아마 석회가 보이는데, 세척 검사를 하지 않을 수는 없다고 생각합니다.
Thyroid nodules are a very common that can be detected in up to 2/3rds of people, often on a physical examination or a test done for other reasons. While most thyroid nodules are not cancer (benign), ~5% are cancerous. Thus, clinicians are often faced with the task of deciding which nodules require further investigation for thyroid cancer with a biopsy, and which nodules can be followed by just observation. In this respect, thyroid ultrasound is the best imaging test to evaluate thyroid nodules, because it can detect features that are felt to predict cancer.One of the most important ultrasound features of cancer is the presence of calcifications, especially microcalcifications, in a thyroid nodule. Microcalcifications within a nodule are small flecks of calcification 1 mm or less in size that appear bright on an ultrasound image. In contrast, macrocalcifications are more coarse areas of calcification that are greater than 1 mm in size. The presence of microcalcifications (and not macrocalcifications) on an ultrasound is felt to be highly suggestive of thyroid cancer because they are assumed to correlate with the round, calcified Psammoma bodies of papillary thyroid cancer that a pathologist sees when examining thyroid tissue under a microscope after surgery. Thus, it is commonly accepted that, when present on an ultrasound, microcalcifications represent areas of papillary thyroid cancer. Since calcifications can also be seen in benign thyroid nodules, the aim of the current study was to examine whether ultrasound calcifications truly predict a) calcifications in thyroid tissue itself and b) the diagnosis of papillary thyroid cancer.THE FULL ARTICLE TITLE:Bilici S et al Histopathological investigation of intranodular echogenic foci detected by thyroid ultrasonography. Am J Otolaryngol 2017;38:608-13. Epub July 5, 2017.SUMMARY OF THE STUDYThis study included 81 thyroid nodules from 81 patients who underwent thyroidectomy at a single center in Turkey between January 2013 and March 2014. Patients were included if the same ultrasound features were observed by two different radiologists. The presence of calcifications in both the ultrasound image and the surgical tissue was noted and the relationship between cancer and calcification patterns was determined.Of the 81 patients, 63% were female and the average age was 50 years. Ultrasound calcifications were detected in 42 (51.9%) of all nodules, although only 22 of those (27%) were true microcalcifications and the other 20 (24.7%) were macrocalcifications. Of the 42 nodules with any type of ultrasound calcification, 28 of them (66.7%) actually had calcifications in the tissues examined after surgery. However, only 11 of the 22 nodules (50%) with ultrasound microcalcifications contained calcifications in the thyroid tissue. In fact, 5 (12.8%) nodules without ultrasound calcifications were found to have calcifications on in the thyroid tissue.Overall 23 of the 42 (54%) nodules with any type of ultrasound calcification were cancer, but 13 of the 29 nodules (45%) without ultrasound calcifications were also found to be cancer. Consequently, the rate of cancer was not different between nodules with or without ultrasound calcifications. Finally, only 12 of the 22 nodules (54%) with microcalcifications on ultrasound were found to be cancer and there was no difference in the rate of thyroid cancer between nodules with ultrasound microcalcifications and macrocalcifications.WHAT ARE THE IMPLICATIONS OF THIS STUDY?Overall patterns of microcalcifications and macrocalcifications seen on ultrasound were only loosely correlated with calcification in thyroid tissue. Furthermore, the presence of either of these types of calcifications did not reliably predict cancer . These results highlight the importance of evaluating multiple criteria for thyroid cancer , including those obtained through clinical history , physical examination and diagnostic
갑상선 거대석회결절(macr ocalcification)
학생 때 그렇게 배웠어요갑상선에 가장 일반적인 유형인 유두상암에 흔히 나타나는 소견이 석회화(미세석회화;microcalcification)라고 하는 것으로 갑상선에 석회화 결절은 암일 가능성이 높기 때문에 반드시 세포검사를 하도록
그럼 갑상선에 석회화 결절이 있다고 하면, 암의 확률은 어느 정도일까요?
One of the most important ultrasound features of cancer is the presence of calcifications , especially microcalcifications , in a thyroid nodule . The presence of microcalcifications on an ultrasound is felt to be highly suggestive of thyroid cancer . Since calcifications can also be seen in benign thyr … www.thyroid.org
재미있는 논문이 있어서 가져와봤어요.
- 초음파상 석회가 보여도 조직검사상 석회가 나온 경우는 절반밖에 없는 2.12.8%는 초음파상 석회가 없는데 조직검사상 석회가 있었다.3. 석회가 있는 경우 (미세석회화인지 큰 석회결정인지 관계없이) 54%에서 암이 발견됐다.4.45%는 초음파상 석회가 없었음에도 암이 발견됐다.5. 초음파상 석회가 있는지 없는지는 암 발견율에 관계가 없었다.6. 초음파상 미세석회화가 있는 54%에서 암이 발견되었는데, 이는 거대석회결절과 그 비율에 차이가 없었다.
이 논문이 암시하기를, 석회화는 신뢰할 수 있는 ‘암의 결정적 징후’가 아니라는 것, 특히 미세석회화(microcalcification)가 암과 강한 관련이 있다는 상식은 상식이 아니라는 것입니다.
따라서 저자는 갑상선암을 진단할 때 다양한 상황을 고려해야 한다고 주장하고 있습니다.임상적 양상, 과거사, 영상학적 이미지, 가족력 등 단순히 석회화 하나만으로 단정짓지 말아달라는 것입니다.
하지만 아마 석회가 보이는데, 세척 검사를 하지 않을 수는 없다고 생각합니다.
Thyroid nodules are a very common that can be detected in up to 2/3rds of people, often on a physical examination or a test done for other reasons. While most thyroid nodules are not cancer (benign), ~5% are cancerous. Thus, clinicians are often faced with the task of deciding which nodules require further investigation for thyroid cancer with a biopsy, and which nodules can be followed by just observation. In this respect, thyroid ultrasound is the best imaging test to evaluate thyroid nodules, because it can detect features that are felt to predict cancer.One of the most important ultrasound features of cancer is the presence of calcifications, especially microcalcifications, in a thyroid nodule. Microcalcifications within a nodule are small flecks of calcification 1 mm or less in size that appear bright on an ultrasound image. In contrast, macrocalcifications are more coarse areas of calcification that are greater than 1 mm in size. The presence of microcalcifications (and not macrocalcifications) on an ultrasound is felt to be highly suggestive of thyroid cancer because they are assumed to correlate with the round, calcified Psammoma bodies of papillary thyroid cancer that a pathologist sees when examining thyroid tissue under a microscope after surgery. Thus, it is commonly accepted that, when present on an ultrasound, microcalcifications represent areas of papillary thyroid cancer. Since calcifications can also be seen in benign thyroid nodules, the aim of the current study was to examine whether ultrasound calcifications truly predict a) calcifications in thyroid tissue itself and b) the diagnosis of papillary thyroid cancer.THE FULL ARTICLE TITLE:Bilici S et al Histopathological investigation of intranodular echogenic foci detected by thyroid ultrasonography. Am J Otolaryngol 2017;38:608-13. Epub July 5, 2017.SUMMARY OF THE STUDYThis study included 81 thyroid nodules from 81 patients who underwent thyroidectomy at a single center in Turkey between January 2013 and March 2014. Patients were included if the same ultrasound features were observed by two different radiologists. The presence of calcifications in both the ultrasound image and the surgical tissue was noted and the relationship between cancer and calcification patterns was determined.Of the 81 patients, 63% were female and the average age was 50 years. Ultrasound calcifications were detected in 42 (51.9%) of all nodules, although only 22 of those (27%) were true microcalcifications and the other 20 (24.7%) were macrocalcifications. Of the 42 nodules with any type of ultrasound calcification, 28 of them (66.7%) actually had calcifications in the tissues examined after surgery. However, only 11 of the 22 nodules (50%) with ultrasound microcalcifications contained calcifications in the thyroid tissue. In fact, 5 (12.8%) nodules without ultrasound calcifications were found to have calcifications on in the thyroid tissue.Overall 23 of the 42 (54%) nodules with any type of ultrasound calcification were cancer, but 13 of the 29 nodules (45%) without ultrasound calcifications were also found to be cancer. Consequently, the rate of cancer was not different between nodules with or without ultrasound calcifications. Finally, only 12 of the 22 nodules (54%) with microcalcifications on ultrasound were found to be cancer and there was no difference in the rate of thyroid cancer between nodules with ultrasound microcalcifications and macrocalcifications.WHAT ARE THE IMPLICATIONS OF THIS STUDY?Overall patterns of microcalcifications and macrocalcifications seen on ultrasound were only loosely correlated with calcification in thyroid tissue. Furthermore, the presence of either of these types of calcifications did not reliably predict cancer . These results highlight the importance of evaluating multiple criteria for thyroid cancer , including those obtained through clinical history , physical examination and diagnostic